Last month I posted about holistic care; where was I up to? Yes, of course definitions...
I came across this article that includes reference to Jan Smuts (1926) who is generally attributed with coining the term holism. The article also highlights that holism is often associated with alternative medicine. I'd like to suggest here that holism extends far beyond any specific school of medicine or new ageist theme. A conclusion reached from contemplating the state of the World and using Hodges' model. So let's consider holism as a feature, characteristic or principle of care theory, practice and policy. What follows may well apply generally.
To begin, if health and social care (plus pastoral) is to be person-centred and situated then agency (who) must be a central factor in defining holism - holistic care. Then I would add the concept of information followed closely by knowledge. Stepping back slightly 'holistic' in h2cm denotes openness, inclusiveness and comprehensiveness.
AGENCY: In Hodges' model I think there are four aspects to agency:
- The person who is the 'patient';
- The health / social care agent;
- Others associated with the patient (family/friends as carers);
- The population at large (local, national through global).
The definition of the health care agent can be described as
idealised or
actualised;
implicit or
explicit;
indirect or
direct(?)

Please pardon the verbiage here both that last sentence and the volume. I'm still trying to figure this out. If you hadn't noticed I'm scribbling all this on an envelope. Any assistance or suggestions gratefully received.
A definition needs to account for the way it [holistic care] is used in day-to-day language, across various settings and contexts. To explain a bit more: imagine there is a community service with a multidisciplinary team that is 'holistic' in that it includes all professional (qualified and unqualified) disciplines, and voluntary practitioners of care. In combination this holistic service bring with them a range of knowledge and skills that is comprehensive. There are distinct pools of specialisation, with the inevitable overlap of some skills - otherwise how could people co-work? So on paper this team could - idealistically - be said to be 'holistic'.
If, however, all of these agencies were to be involved in a single case, then another definition of 'holistic care' emerges. This highlights the importance of context on working definitions derived from the service (agent) side, in contrast to definitions from the patient (subject) perspective and policy (Government). If you need some indication for the level at which Hodges' model operates look no further. At this level the patient and informal (family) carers are also agents, supporting the notion of self care.
It could well be that the whole team are legitimately required to respond to a referral, but if not this would constitute a huge waste of resources. The actualised sense of holistic care is expressed in policy - interventions must be commensurate with need. We cannot divorce health care from governance and economics. In fact there may be a case of abuse to answer for. You really can have too much of a good thing.
Point #4 above may seem to stretch the concept of agency too far. Problems first launched in the 19th century are coming home to roost. There is (currently) nowhere to run or fly. The inclusion of local through global sense of agency is a MUST. Patient care is de rigueur, self care is a major challenge*, both are insufficient in terms of achieving holistic care:
Staff: "Always observe discretely and check the welfare and safety of the quiet, withdrawn patients in your care."
Student: "Who's that sat in the corner?"
Staff: "Where? You mean the lady sat in the other corner don't you?"
Student: "Hold on .. why - she's in all four corners, in fact she's everywhere..."
Staff: "Oh, yes that's right her name's Mrs Green and actually she's not so quiet these days. It's all very sad. We're trying to include her in things."
Student: "What's the problem?"
Staff: "Some very complicated and damaging relationship problems, gross personal assaults of the worst kind that we can't discuss here, but the lawyers are talking about crimes against humanity.... All her children are threatened. Goodness is that the time! Is it time for your break? Perhaps you could go try and speak to her. Better still maybe just listen..."
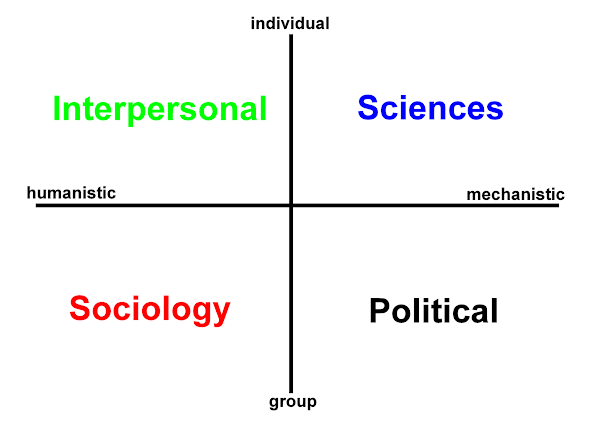
INFORMATION: If agency is primarily centred on the left side of
h2cm namely the humanistic axis with the INTERPERSONAL & SOCIOLOGAL domains - then this needs to be counterbalanced if the model is to mean something. ICT (information and communication technology) IS an essential factor.

For our purposes though we need to fracture this union and separate out information, communication and technology
(Intensely Confusing Terminology?).
If we untie the digital knot, then we can better reflect upon the sociotechnical dimensions of holistic care.
KNOWLEDGE: This brings us to the next definition that can be built on conceptual and prepositional foundations. A definition of
holistic care relating to knowledge can (surprise-surprise) also utilise Hodges' model.
I've to pull-the-plug somewhere - sorry info and know are very brief. Thanks for stopping by awhile, safe travels until we meet again at this crossroads.
I hope you'll be back and that these reflections are helpful?
More to follow: Holistic care No. 3: Location
holism:
Smuts, J.C. (1926) Holism and evolution. New York: Macmillan.
*The real challenge is avoiding the need for self-care!














 orcid.org/0000-0002-0192-8965
orcid.org/0000-0002-0192-8965