Holistic Bandwidth [I] - Where's the brush?
Apart from those intervals and instances (times!) when emergency intervention is needed, holistic care is seen as a primary goal in health and social care theory, practice and policy.
IF care is not holistic THEN it could be argued that there is care dissonance.
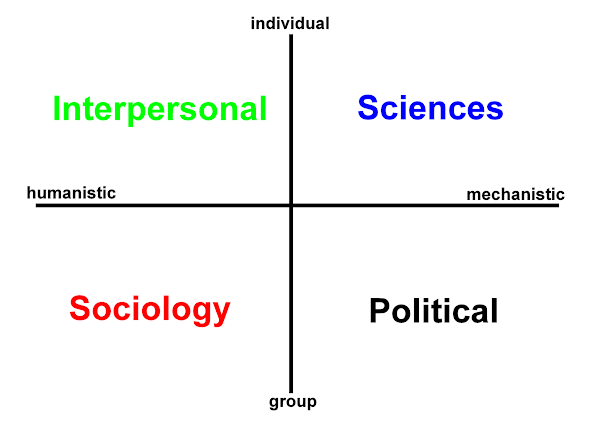
The high quality non-critical, general efforts in the PHYSICAL [SCIENCES] care domain -
fluids, diet, warmth, pressure sore care, comfort, security, infection control ....
can be compromised by lack of attention to the EMOTIONAL [Intra-INTERPERSONAL] care domain -
respect, empathy, unconditional +ve regard, non-judgemental attitude, time, space, attention ....
- what the patient (carers and others*) expect to follow does not occur.
 Rather like cognitive dissonance acute discomfort results when care of the required high quality (holistic, timely, person-centred...) is not applied across the board (h2cm).
Rather like cognitive dissonance acute discomfort results when care of the required high quality (holistic, timely, person-centred...) is not applied across the board (h2cm).
(In being human) everyone recognises the BASICs of CARE (discuss?):
Remembering demands an assured space in the organisational memory - such that staff in those other spaces - wards, clinics, patient's homes, residential homes are able to fulfil the holistic spectrum of care needs.
Dissonance encourages game playing with beliefs [1-n players].
It is very easy and a fairly well understood human trait for us to become pre-occupied with what we do. (As you will have noticed I have a problem with brackets and italics...) When at work (i.e. not day-dreaming) "It is what we do that counts."; but care variances bound to professional disciplines and particular clinical settings should not be wielded as a foil.
So, perhaps this dissonance can be represented as distance:
- patients and carers may not articulate their discomfort - at the time
- as the distance between concepts and their meanings.
more to follow....
I Googled 'organisational dementia' and found the following reference:
‘Sustaining New Industrial Relations in the Public Sector: The politics of trust and co-operation in the context of organisational dementia and disarticulation’ (with M. Martinez Lucio), in P. Dibben, P. James, I. Roper, and G. Wood (eds.) Modernising Work in Public Services London: Macmillan. 2007.
*There is probably a major cost on staff morale here also.
![]()

 orcid.org/0000-0002-0192-8965
orcid.org/0000-0002-0192-8965