Nursing human rights - dementia care II: fao Sir Gerry Robinson
The 2nd and final edition of BBC Two's TV programs Can Gerry Robinson Fix Dementia Care Homes? was on last night and made for uneasy viewing.
The saving grace for the public's confidence (if there is one) was repetition of the excellent care at one home.
For all the negatives presented on TV, before mapping the key content of this program using Hodges' model it must be acknowledged that the staff and both managers involved are to be congratulated in allowing and facilitating the production of this program. Sir Gerry and the program's producer(s) obviously travelled an especially difficult course in this episode.
Unless qualified or having undergone some training, many staff will behave and eventually modify their norms and expectations according to what they are exposed to within a short period of starting to work in residential care. Perhaps, this explains in part the adage 'start as you mean to go on'? It was apparent that many staff knew they were failing, they recognised the lack of leadership, their inability to sustain the effort for positive change.
This is why (in 1977 at least) the school of nursing I attended was a little more than churlish about students initially working as a nursing assistant. If you were not working on a ward that also trained student nurses then you may adopt the wrong attitudes and with it what we might call 'non-skills'. This includes 'learning' means of avoiding contact and interaction with patients; and possibly interpreting behaviour in a purely negative and non-therapeutic way. This may extend to the point of becoming personally involved - taking things personally - whether the behaviour exhibited is aggression or sexual dis-inhibition, for example.
Here then are some of the points I noted, many are repeated from the first program with some very unfortunate and troubling additions (which I may further review as per the above text):
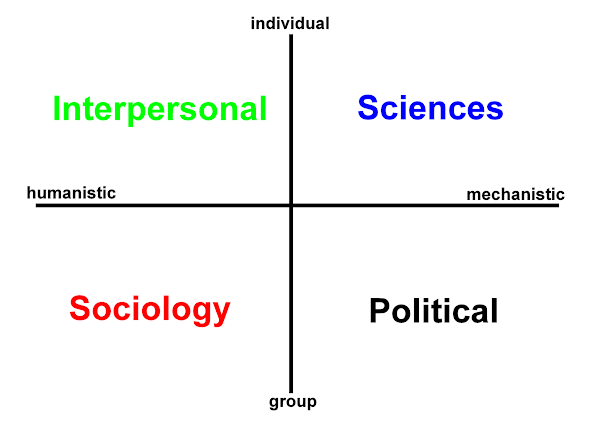
| PURPOSE, CARE PHILOSOPHY (none?), person-centered care, attitude, memory loss, vulnerable individuals, training, risk, assessment, motivation to change, interpersonal skills, motivation, listening, life skills, knowledge and skills, feedback, aggression, agitation, measures, rapport, empathy, +ve care, boredom, personal choice & autonomy, access to personal belongings, dolls, personal focus, anxiety, psychological stress and trauma of physical relocation | physical environment, colour, decor, noise, outside access - physical security, physical restraint - use of furniture, position of furniture, day-to-day items, tasks, PROCESS, measures 'dementia care mapping', routine tasks, time with residents, assessment, care files (paper!), bed occupancy, activities - painting, gardening, sheds, staffing cover : resident ratios, models of care (none?), objective measures |
| PRACTICE (common minimum standards), the residents, team work, day staff:night staff, collective faith and trust, collaborative objectives, care, shared enthusiasm, social attitudes, dignity and respect, relationships, social values, personal-social history, engaged activities, involvement, 'social' norms, inclusion, community - institution, being valued by others, impact on families and local community of home closure | POLICY (the lines in the sand?), management spot checks, '24 hour care', disciplinary procedures, professionalism in management relationships, duty of care, ratings: tokenistic inspection regime, home closure, consultancy, audit, legislation, sickness, pay, business ethos, staff morale, recruitment and retention, confidentiality, sanctions, management style, qualifications, standards, institutionalised care, re-location, lessons learned (business involved, local authority)? |
There are also Open University learning resources associated with the program.
My closing thought: in closing the asylums over the past 40+ years I hope we have not and are not creating a series of micro-institutionalised replacements.
![]()

 orcid.org/0000-0002-0192-8965
orcid.org/0000-0002-0192-8965