Evidence Based Medicine & Care and the I-G Nexus
Great store is placed upon evidence based medicine (EBM), nursing and care. There are dedicated centers, conferences, journals, policy pronouncements and much more besides.
 The evidence based approach has been subjected to critical review in leading health, medical and research journals and blogs. The status and presence of EBM as the bridge between clinical theory and practice is not in question, it is only right however that nothing is taken for granted. EBM is not necessarily as scientific - as objective - as the clinical trials and meta-analyses... make it appear.
The evidence based approach has been subjected to critical review in leading health, medical and research journals and blogs. The status and presence of EBM as the bridge between clinical theory and practice is not in question, it is only right however that nothing is taken for granted. EBM is not necessarily as scientific - as objective - as the clinical trials and meta-analyses... make it appear.
Dr Nicholas Hicks provides a brief and yet informative piece on the definition and scope of evidence based health care on Bandolier.
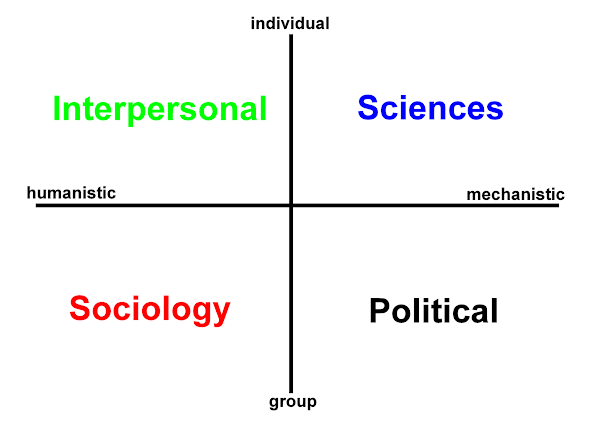
The success of EBM depends however on the GROUP: the sensitive aggregation of results with the personal details stripped out (anonymised). EBM is still (rightly) subject to debate, its method and methodologies constantly scrutinised. In terms of contemplating the complete care spectrum Hodges' model places the natural home of EBM as being grounded in the SCIENCES domain. The POLITICAL domain provides a vital, supportive and reinforcing role through policy, governance and reporting, nationally and internationally. Subsequent studies are modified and refined to ensure lessons are learned.
The ongoing challenge that the application of EBM&HC presents can be found in h2cm, if we choose to reflect there. What we must never forget is that the benefits of EBM are delivered to INDIVIDUALS. Ultimately, it is they who benefit from improvements in treatments and care. It is the individual who remains at the centre of care.
"Evidence based" approaches are being applied in a great many disciplines, but it is the notion of EB care (EBC) as Hicks writes that deserves our special attention. Thinking back to basic physical nursing care c. late 1970s: whilst the best treatment for pressure sores is prevention, this is one area that has benefited enormously from evidence based research. For decades pressure sore treatment and care variously relied upon custom and practice, the myth of Sister x, y, z (or "we do it this way..."), to scientific scramblings, argument and debate.
EBM has recognised the need for quality as well as quantity.
There may also be a stark contrast between the time-scales of EBM and EBC?
If we split "EB" and the "C", we see that there is a danger that the 'I' may get lost:
- To what extent is EBM situated, such that the patient would also recognise the context?
- To what extent is EB(x) a baton for best practice? -
- That is, from the start lines in research lectures, learned journals, research supervision and international study centres - how easily is EB(x) transferred to wards and other clinical areas? (Having 'best practice' examples is the just the start: how will these be communicated?)
- Are the notions of 'holistic assurance and bandwidth' applicable and of value here?
- Is EBC patient AND staff empowering? Is EBC like EBM supported by the underlying (political domain's) foundation of policy and audit to ensure that change does happen and staff can deliver safer, more effective, individualised, person-centred care?
 The best evidence is that gleaned from the source. This does mean the non-trivial task of juggling subjective and objective health. It means engaging with the patient and community. It means that the best evidence for care should also be timely. This may be a fuzzy form of EB(x), but in contrast to the steel bearing that EBM can often present, there are plenty of hooks that can make a real difference.
The best evidence is that gleaned from the source. This does mean the non-trivial task of juggling subjective and objective health. It means engaging with the patient and community. It means that the best evidence for care should also be timely. This may be a fuzzy form of EB(x), but in contrast to the steel bearing that EBM can often present, there are plenty of hooks that can make a real difference.Source:
Sullivan, M. (2003). The new subjective medicine: taking the patient's point of view on health care and health. Soc. Sci. Med. 56(7), 1595-604.
Image sources:
(were listed.)
![]()

 orcid.org/0000-0002-0192-8965
orcid.org/0000-0002-0192-8965