Relative poverty (2) - political
[The introduction is repeated across these posts: intrapersonal, sciences, sociology]
There are many paradoxes in life and many are concentrated in the realm of health and medicine (the major sub-division of life and death).
For decades the link between poverty and standards and quality of health has been recognised and politicised in the media and policy. Just this past week was news of a Bill to make the eradication of child poverty a legal obligation not something that can be the political objective at the start of a Government and then cast aside.
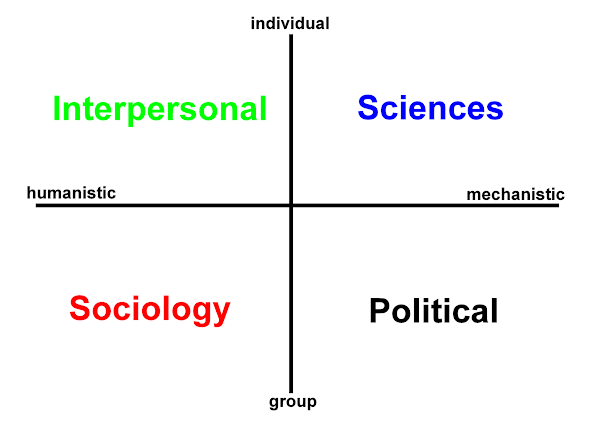
Many things are relative and poverty is often described in this way applying to individuals, social classes, communities, regions and whole nations. Using the domains of Hodges' model what reflections does this prompt? Let us see:
POLITICAL: Although we are told that change is happening swathes of humanity face -
 There are those who are able to decide and yet denied choice due to a politics or state that spits explicit corruption denying the people their expressed and collective will. Although previously described as 'black and white' politics must become participative AND must become 'green and (truly) global'. As events in 2009 attest here in the UK, politicians, those key workers / case practitioners in this domain (should paradoxically) disavow personal ambition and at times yet to be decided the party whip system. Yes, these matter, but again space (vacancy) is needed to accommodate - permit and facilitate true focus.
There are those who are able to decide and yet denied choice due to a politics or state that spits explicit corruption denying the people their expressed and collective will. Although previously described as 'black and white' politics must become participative AND must become 'green and (truly) global'. As events in 2009 attest here in the UK, politicians, those key workers / case practitioners in this domain (should paradoxically) disavow personal ambition and at times yet to be decided the party whip system. Yes, these matter, but again space (vacancy) is needed to accommodate - permit and facilitate true focus.This is no chance opposition of domains in Hodges model.
is mediated through the social domain.
Like health professionals, politicians and civil servants must wipe the slate clean: constantly. This is why transparency in politics is so crucial to trust, engagement, and grounded politics. ...
'P' is for politicians not just the 'people'.
Politicians need to be engaged coherently.
Touch is the interface for them too.
A week is a long time in politics because the sun never shines (not even in 'victory'). For these people being open, transparent, non-judgemental ... means their vision is refreshed by a perpetual rain.
even if poverty and even more so if poverty
represents where they came from ...
Image source: Equator Network
Additional links:
Reith Lectures 2009 BBC 'A New Citizenship'
'Poverty' on W2tQ
Political care (knowledge) domain links resource
![]()











 orcid.org/0000-0002-0192-8965
orcid.org/0000-0002-0192-8965