The following e-mail was received this week from (Prof.) George Kernohan and includes correspondence with Mary A. Waldron, Research Assistant, University of Ulster (thanks to Mary for confirming the reference).
My responses to George's points are right justified, italicised.
<->
Peter,
I am beginning to find examples of Hodges’ model every day now.
Once you adopt the model as a framework George it does tend to frame everything,
so I am not surprised at your finding. Maybe there is a paper there too...
Today we had a second research meeting to consider a (more) rigorous attempt to evaluate the provision of ‘support’ to carers of people undergoing palliative or End-of-Life Care (EOLC). An area of care with a dearth of evidence. So we looked at one review from Grande et al. (2009). They say that:
There has already been considerable research identifying carers’ needs in EOLC. These include psychological support, information, help with personal, nursing and medical care of the patient, out of hours and night support, respite, domestic and financial help.9,10,16–21 There is also a large body of research into adverse effects of care-giving, such as anxiety, depression, stress, strain, fatigue and mortality.22–24
Given this strong evidence base, any further investigation into the prevalence of needs and adverse effects should mainly focus on under-researched groups to ensure that future interventions are sensitive to their specific concerns. This includes carers of patients with conditions other than cancer, including neurodegenerative disorders,25 respiratory26 and cardiovascular diseases,27 to help us understand how differences in disease trajectories, awareness of the terminal nature of the disease and available support28 translate into different carer experiences. Although carers of patients with dementia have been extensively researched, little is known about their needs during patients’ final phase of life.9 p.340.
(The numbers refer to references by Grande et al., I have extended the quote used here).
Thanks for this paper George (and Mary) which I will read in full.
I extended your quote to encompass some additional interesting ideas.
To move toward a plan for a more rigorous evaluation, I would like to use a simple framework: here we go!
I think I will be suggesting Hodges’ Health Career as a possible model.
:-) ! If I can support you in this George I am pleased to help.
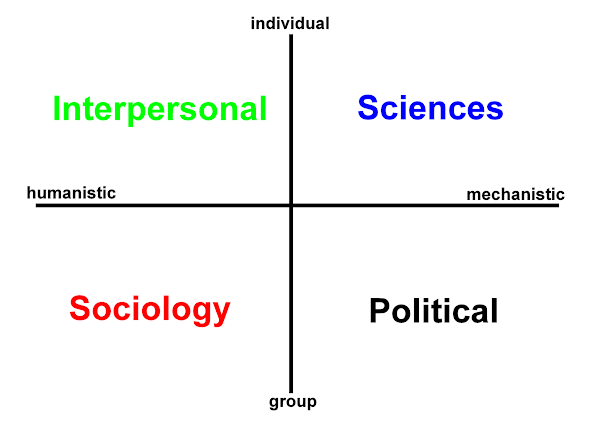
This could provide a framework for all carer-focused interventions in a broad way. As always, it would imply that carers need to have their needs addressed in terms of science, sociology, politics and interpersonal needs. As I see it, the first step would be to ‘map’ the carers’ needs onto that framework (from publications, if necessary from carers themselves). The basic idea (I think) is that care should address the four quadrants:
- Science: (carer’s physical needs, information, instruction)
- Political: (policy that enables care for carer, finance, allowance)
- Sociology: (recognising that people need people, networks and “sharing” groups, story telling/hearing)
- Interpersonal: (psychological support, prevention of anxiety & depression)
Have you any thoughts or guidance on this “mapping exercise”?
Goodness, that's quite a question!
Plenty of thoughts George but not sure how meaningful ....
Basically, since a community mental health project in 1990s
I have always considered (as per standard approach of course) that a toolkit of measures are needed. Even when we start from that most basic of distinctions between
demand and
supply.
As per your approach if h2cm is considered as a circle, a spectrum -
(sometimes we must circle the square)
then (if holstic) the adopted measures should cover all the domains:
Political: (outcomes, carer, patient satisfaction, financial assessment (means testing), respite care frequencies, reviews)
Interpersonal: (mood, coping ability, anxiety, depression, sleep, HoNOS)
Sciences: (pain, general health scales, care complexity (measures?))
Sociology: (dedicated carer assessment tools, sociability - social network size, psychosocial measures... there are many out there)
George, I realise the above is a ragbag collection but - like yours - these are dimensions which can (must) be reduced. Now there is also emphasis on this area post Darzi and the 'new' quality agenda.
This will serve (and is serving) to emphasize the distinctions between measures:
Objective - Subjective
Quantity - Quality
Staff administered - Self (Patient, Carer) administered
Global/general - condition specific
Service centered: Primary care - Secondary care
While it is easy to spin dichotomies,
the NHS must (constantly) focus on this area whatever the policy emphasis:

NHS Information Centre: Measuring for Quality Improvement
NHS Information Center: What is happening on indicators for...?
NHS Inst. for Innovation and Improvement: Quality and Service Improvement Tools
Earlier this year I contacted the NHS-IC [enquiries at ic.nhs.uk] regards additional measures of quality suggesting that the health career model bears due consideration (research).
Mental health services (and others?) have recognised how the measures they use can be a chaotic, personally selected, preferred, legacy-mix of assessment tools. Dictated by Senior Nurses, Consultants, Senior Management and not the evidence base. Now these are assured (are they?) with purposed selection (a task worthy of an 'away day') and then supported with regular in-house training.
Last month Anne-Marie Osbourne-Fitzgerald, Clinical Development Nurse, with (her) Clinical Manager, Denise Banks (Cygnet Hospitals), met Michael Doyle (Univ. of Manchester & Edenfield Unit, Prestwich Hospital) and I one evening at the Trafford Center in Manchester. Our two hour+ discussion covered the health career model, documentation, approaches to formal assessment and future plans (aspirations!). In the time available we obviously only scratched the surface, but Mike and Anne-Marie brought along examples of their paperwork.
Mike demonstrated how the health career model can be used implicitly or explicitly. At the Edenfield Unit the domains are being used individually to make up what is a standard A4 portrait form. The model informs their existing documentation; rather than the explicit form of the h2cm with the 2 x 2 matrix.
(I have a MS Word version of the latter and must update this to other formats).
Legally, as we know if it is not written down, recorded then it did not happen.
Educationally however, the objective is
also to get students - practitioners -
to think - before they do.

Anne Marie's documentation example at Cygnet Hospital included The Recovery Star:
http://www.mhpf.org.uk/recoveryStarApproach.asp
As you consider the star's points against the domains of the health career model - where in the model are you?
Can this provide another means to define 'care pathway'? A way that is not masked, hiding behind political, policy rhetoric (and really service-centered)? There are without question some excellent tools available, so care needs to be taken not to re-invent the wheel - hence your literature search. In some tools the effort and engagement of patients, carers and the public is exemplary. It seems what is needed is a hybrid solution. There is no single measure.
It may not sound scientific, but the complexities of care mean that academics, clinicians and managers must resort to a pick'n'mix approach. There is a battery of evidenced tools each with their history, application context and issues log (Why not? Lack of the latter might denote that such tools are no longer in development / review). As a clinician also involved in training, managers need to listen and make some tough operational decisions. The comms 'traffic' between clinicians, their managers, and senior managers needs to improve even more. Since, just using the above as an example, the STAR approach may find us on a ramble in the humanistic domains, the constraints of the mechanistic domain prompts the clinician's to ask:
"If you want me to use this assessment tool, what other thing do you want me to put down?"
As we are all aware: There is only so much time in a day, week, month, quarter. ...

In follow up emails I directed Anne-Marie to -
http://www.p-jones.demon.co.uk/contexts.htm
If you scroll down there is some discussion and graphics I did quite a while ago. This deserves revision as per the rest of the website, but the ideas are there I believe which can inform your project George?
Back then - and here on W2tQ I have been trying to demonstrate the wide range of contexts to which the health career model can be applied. In our meeting that evening the well established Tidal Model was also noted. This has of course benefitted from specific development, as per research that has produced audit and evaluation tools (
Stevenson, et al. 2002).
It might make a useful reflective article – or at least a conference presentation. Ideally it would lead us to a measurement or observation approach ...

I would relish the prospect of a paper George, or a conference presentation. Not just contributing as a co-author/presenter, but supporting and enthusing new authors. The 21st century belongs to our students. Hodges' model can act as 'stellar' nursery not just here in the UK and EU, but globally. And not just in our respective disciplines
(mental health, palliative - end of life care, forensic nursing care), but in informatics - conjoining and championing the need for socio-technical perspectives.
In addition to the above and
thinking before they do, all health and social care practitioners
must be able to reflect
after.
As one of the original purposes for the model in my initial interviews with Brian Hodges (1997-98), research work addressing these are much needed.
This conceptual framework can offer much in case formulation, evaluation, clinical supervision, patient, carer and public (health) engagement.
[In short -] Can we measure Hodges' model?
George K. (Prof.)
You started with a big question George and similarly here at the end.
We have to be able to do this. In the first instance taking apart your question - there are clearly several questions here:
PRACTICE:
Above you noted that:
This could provide a framework for all carer-focused interventions in a broad way. As always, it would imply that carers need to have their needs addressed in terms of science, sociology, politics and interpersonal needs. As I see it, the first step would be to ‘map’ the carers’ needs onto that framework (from publications, if necessary from carers themselves).
It would be interesting to consider the formal process and practice of dementia care mapping against Hodges' model. Perhaps the approach you seek is something similar? If carer's make use of self-assessments these e-documents might act as an input for text analysis tools? If appropriate you could also weight certain items according to the priorities of carers? This would build on other carer research adding validity to your 'final' objectives.
Carers and clients (patients, service users) can with due explanation, appreciate the health career model. The model has a role to play in health education. I can well imagine a proforma similar to the Recovery Star example above, but purposed for carers and underpinned with the health career model. We also need to remember the spiritual domain, which is collective.
Ultimately George, your question concerns our ability to measure holistic, integrated, person-centred, multidisciplinary care and to state the obvious: there is no single measure to do this. Several tools and approaches gathered within a conceptual framework might however provide an environment favourable for a hybrid measure to emerge - literally a cycle?
THEORY:
In the paper you referred to George - Grande. et al. (2009) state:
In parallel with the lack of empirical evidence, there has been a lack of theoretical and conceptual models for when and how support provision in EOLC should improve carer outcomes. To guide further research, palliative care may here benefit from drawing on models within other fields, such as gerontology, sociology or psychology. p.341.
I am biased, but reading the paper the potential of the health career model as a high level tool is convincing just from a 'disciplinary cross-match'. Intra-, interdisciplinary, metadisciplinary and transdisciplinary perspectives could be a focus. This in addition to the specific knowledge and practical domains of sociology and psychology and as the authors note models therein. I forget the reference at the moment (and will check), but I recall carers / family units being framed in terms of strengths and weaknesses. That is, events, characteristics and relationships impact on a family with either additive, subtractive or neutral effects. This would seem applicable here?
While Grande et al. (2009) note that the (informal) carer's role is hidden (and is routinely described in this way) I wonder if in palliative care there are other dimensions that accentuate this 'hidden, covert' role?
The politics of potential death and actual dying may be another factor the health career model can help illuminate in a constructive, enabling way? Health care, patiency, sick roles, caring are always mediated by 'politics'. Hence the need for a political domain in any conceptual framework that Grande, et al. may consider. On a negative front, the model might also illustrate alienation and related concepts?
In conclusion!
Thank you so much George and Mary for my being able to share your initial thoughts here and respond with some of my own. I hope this helps you take your work further? There may be a few points to follow, which I will add and as you have noted above there is much that could be done to take this further.
Peter J.
From: Waldron Mary [mailto:MA.Waldron at ulster.ac.uk]
Sent: 06 June 2010 17:49
To: wg.kernohan at ulster.ac.uk
Subject: Carers Support Evidence
George,
Jury's still out on the effectiveness of support interventions and programmes which support carers in palliative care. Not enough research. Lack of evaluation, lack of rigour, no conclusive research, but lots of policy advocacy of carers support and addressing of needs. Sample of lit attached.
Mary A Waldron,
Research Assistant,
School of Nursing,
University of Ulster.
Many thanks George and Mary for your ongoing interest, and to Anne-Marie, Denise and Mike.
Reference:
Grande, G. et al. (2009) Supporting lay carers in end of life care: current gaps and future priorities, Palliative Medicine, 23: pp. 339-344. DOI: 10.1177/0269216309104875
Stevenson C, Barker P and Fletcher E (2002) Judgement days: developing an evaluation for an innovative nursing model. J Psychiatric and Mental Health Nursing, 9(3), 271-276.
Stellar nursery image
My source: http://media-2.web.britannica.com/eb-media/60/21260-004-3C62CA58.jpg









 orcid.org/0000-0002-0192-8965
orcid.org/0000-0002-0192-8965