Hodges' model is a conceptual framework to support reflection and critical thinking. Situated, the model can help integrate all disciplines (academic and professional). Amid news items, are posts that illustrate the scope and application of the model. A bibliography and A4 template are provided in the sidebar. Welcome to the QUAD ...
buses - Eddie Stobart - Lego space - time 1-day Physical care Another day the sound of laughter
Source: Twi/X + image:
Whistlestop London visit for @JSTheatre#LaughingBoy, a complete must watch. So lovely to meet the cast and behind the scenes magicians, and see so many #JusticeforLB’ers in the flesh.
"Netflix has collaborated with A24, Motive Films, Ventureland and Raw on this gripping look at the undeniable connection forged between two athletes as they navigate the vigorous and competitive world of freediving. The Deepest Breath will have its world premiere at the Sundance Film Festival in January 2023. Logline: A champion freediver trains to break a world record with the help of an expert safety diver, and the two form an emotional bond that feels like fate. This heart-stopping film follows the paths they took to meet at the pinnacle of the freediving world, documenting the thrilling rewards – and inescapable risks – of chasing a dream through the silent depths of the ocean."
ARE YOU WORKING IN THE NHS? IF SO, HELP NEEDED URGENTLY!
Please read this email.
Glasgow Caledonian University is inviting NHS Staff across the UK to participate in this doctoral research survey to analyse the impact of responsible leadership on improving well-being and organisational trust among NHS Staff members.
To be eligible, you must be an NHS staff member from any area of the UK in any job role. The survey collects no recognisable information and is wholly anonymised to protect participant privacy and confidentiality. It has received full ethical approval, will take around 10 minutes and will help provide an improved understanding of the area of well-being in the profession.
Please forward this survey link to everyone in your contacts working for NHS. This will help gain more responses, increasing the study's reach and validity. Your help is highly appreciated, and we thank you in advance.
Here's the link for the participant information sheet and survey:
Bioscape. Incredible whole Beautiful mote - in my eye?
Are your - dreamscapes - yours?
Your inscape alone:
mindscape - your inner eye?
Landscapes, seascapes, skyscapes, spacescapes speak to us. Everyone. Stories of deep time. Stories of truth and truth emerging.
See both sides of the cloudscape. Snowscapes in retreat. Cityscapes on the march. Yes! No! Yes! No! Yes! ... Soundscape*
The sums have it.
What tablescape awaits us?
For us - no escape.
*gone quiet.
My prompt:
Esslin, Martin. Chapter 1 Samuel Beckett, The search for the self. The Theatre of the Absurd. London: Pelican, 1982. (3rd Ed.). p.84. ('psychological inscape')
The increasing availability of digital data, along with recent developments in Artificial Intelligence, especially in the Machine Learning and Deep Learning fields, led the scientific community to debate whether data alone is sufficient for decision making and scientific exploration. We focus the attention on the healthcare domain, where peculiar issues affect data: indeed, data are usually collected under heterogeneous conditions (i.e., different populations, regimes, and sampling methods), suffer missingness – very often not at random – and their use is strongly constrained by privacy issues. In such a complex setting, this special issue challenges computer scientists to contribute to the above debate by designing and developing innovative methodological approaches, for solving complex decision-making problems in health care, leveraging on observational data.
Topics of interest include, but are not limited to, the following with an emphasis on novel generalizable methods applied to the healthcare domain:
Causal discovery from multiple data sets.
Federated causal discovery.
Causal discovery from heterogeneous data sets.
Transportability of causal models and inference.
Neuro-symbolic approaches to learn from heterogeneous data sources.
Continual learning on streams from multiple data sources.
Computational intelligent strategies to support causal inference.
Edge computing for decision making in healthcare.
Integrative AI methodologies.
Distributed inference methods.
Continual Learning.
Knowledge Discovery and Integration.
Combination of deductive approaches with ML models.
Combination of ontologies and/or knowledge-bases with ML to support decision making.
Peer Review Process:
All submitted papers will undergo a rigorous peer-review process featuring at least two reviewers. All submissions should follow the guidelines for authors available at the Journal of Biomedical Informatics website (http://www.elsevier.com/locate/yjbin). JBI’s editorial policy outlined on that page will be strictly enforced by special issue reviewers.
Note that JBI emphasizes the publication of papers that introduce innovative and generalizable methods of interest to the informatics community. Specific applications can be described to motivate the methodology being introduced, but papers that focus solely on a specific application are not suitable. A few examples of papers focused on methods previously published in JBI include: Kyrimi, et al. [1], Huang, et al. [2], Kocbek et al. [3], Houston et al. [4], García Del Valle et al. [5], Graudenzi et al. [6] and Sims et al. [7].
In particular, the authors of [1] showed the relevance of causal models and expert knowledge to develop credible models, i.e., capable of achieving good predictive performances when transported from the study cohort to the target population. Furthermore, [2] tackles the relevant issue of partially overlapping variables when data are collected from multiple data sources. This problem is extremely relevant both in theoretical and practical terms for decision making in the healthcare sector.
The contribution provided in [3] stressed the importance of working in a multi-source context by demonstrating how the linking of different repositories can improve the overall understanding of patients' conditions. Similarly, in [4] the authors extended this concept by introducing a methodology to evaluate to audit the data quality of the sources exploited by healthcare information systems. Then, in [5] the multi-source concept is transferred within the multi-modal environment and the authors surveyed the importance of considering different modalities to obtain a better disease understanding.
The works in [6] and [7] focuses on the importance of data. In [6] a data integration framework is defined for characterizing the metabolic deregulations that distinguish cancer phenotypes, by projecting RNA-seq data onto metabolic networks without the need for metabolic measurements; in [7] a biomedical informatics method is introduced that uses multiple public health data sources to perform surveillance of methadone-related adverse drug events. Interestingly, even if patient data are not linked between different data sources, results show that the integration of multiple public data sources can capture more cases and provide more clinical details than individual data sources alone.
Key requirements for JBI ML papers in addition to presenting novel methods (not simply application of existing methods to a new healthcare domain) are as follows: 1) projects must have clinicians involved in research question/problem formulation, defining input data, and assessing the results. 2) An explanation (with clinicians) of how the proposed method would fit into the clinical workflow is expected. It must be translational to practice. 3) Data sets should preferably be collected from hospitals after the research question was formulated, thus avoiding the use of available data (MIMIC) to define a very wide research problem that could potentially be answered with available open datasets (as an example: detecting if someone has COVID from Chest X-Rays would not be acceptable, as the gold standard test is the laboratory test). 4) As for explainability, SHAP values and related diagrams would not be enough: the paper should clearly describe and explain how clinicians use the visualization to make decisions. For further details please refer tohttps://www.sciencedirect.com/journal/journal-of-biomedical-informatics/publish/guide-for-authors.
The Middle East is a region of both severe water problems, and acute political instability. But what is the relationship between these two things? This Policy Dialogue will provide an opportunity to reflect on this question and its implications. It will overview the region’s water problems, and consider how these problems are – or are not – contributing to conflict. It will also examine, conversely, how war and violence are affecting patterns of water resource degradation and water insecurities, and will reflect on opportunities for water-related peace-building, including on how water for peace initiatives might best be pursued.
We are delighted to invite Natasha Carmi (Water Peace Programme Manager at the Geneva Water Hub) and Jan Selby (Professor of International Politics and Climate Change at the University of Leeds, UK) to share their expertise during this session.
We invite you to join us and explore the complexities of this extremely important issue. You can register here. Please also share this invitation within your networks.
Best regards, Aeve
Aeve Ribbons she/her
Educational Projects Manager of JHU-UPF Public Policy Center (UPF-BSM) Managing Editor of the International Journal of Social Determinants of Health and Health Services (IJSDOHS)
My working days are Monday-Thursday / Mis días laborables son de lunes a jueves.
"Classical psychodrama requires five instruments, the stage, the subject, the director, the auxiliary egos and the audience. Although Moreno frequently stated that psychodrama could take place in many natural settings, he advocated the use of a stage of his own design, circular, 12-15 feet in diameter, 1-2 feet high with two surrounding stepped lower levels, seating for the audience, a 'Juliet' gallery and equipment for varying the colour and brightness of the lighting. This format was was aimed at providing a space and generating an atmosphere in which the subject could rise up to move and act with increased freedom and imagination.
'The locus of a psychodrama, if necessary, may be designated everywhere, wherever the patients are, the field of battle, the class-room or the private home. But the ultimate resolution of deep mental conflicts requires an objective setting, the therapeutic theatre. ...'". p.107-108.
Davies, M.H. Dramatherapy and Psychodrama, Chap. 5. pp.104-123. In Jennings, S. (Ed.), (1987) Dramatherapy. Theory and Practice for Teachers and Clinicians. Routledge, London. p.106.
"... Moreno soon began to seek ways of measuring the form and structure of relationships in groups. The techniques of sociometry which he invented have since been widely and successfully adopted by his successors, becoming an accepted field of social research in their own right. At its simplest, this approach relies on asking of the social grouping under investigation to indicate their relationship to each other so that, for example, a pattern of dominance (vertical structure) or affinity (horizontal structure) can be discerned. These measures may be committed to paper in diagram form (a sociogram) or expressed by the individuals arranging themselves in positions symbolising their relationships (an action sociogram)". p.106.
"More complicated interconnections and patterns can be demonstrated and the group asked to explore alternatives in order to recognise sources of conflict and misunderstanding and to modify them. Moreno foresaw a new discipline for which he coined the name 'sociatry' in which the social organisation rather than the individual is the object of the healer's endeavours, a truly 'group' psychotherapy". p.106.
Anticipating future theory-practice policy and education change.
Could the reduction in the options for student mental health nursing placements be compensated in-part by addressing the concurrent change in the range of therapeutic (modalities) interventions available?
Davies, M.H. Dramatherapy and Psychodrama, Chap. 5. pp.104-123. In Jennings, S. (Ed.), (1987) Dramatherapy. Theory and Practice for Teachers and Clinicians. Routledge, London. p.106.
".. it is the experience of our own wounding that will enable us to engage with our clients in a healing process". p.15.
"Therefore we can begin to understand that rather than the drama being the chaos, the drama is both the container of the chaos and the means of exploring it. Accompanying our groups through such dangerous territory may seem too frightening for the dramatherapist to contemplate, let alone the client". p.15.
"The attributes of liminality or of liminal personae (threshold people) are necessarily ambiguous, since this condition and these people elude or slip through the network of classifications that normally locate places and position in cultural space. Liminal entities are neither here nor there: they are betwixt and between the positions assigned and arrayed by law, custom, convention and ceremonial. As such their ambiguous and indeterminate attributes are expressed by a rich variety of symbols in the many societies that ritualise social and cultural transitions. This liminality is likened frequently to - death, being in the womb, to invisibility, to darkness, to bisexuality, to the wilderness and to an eclipse of the sun or the moon". p.14.
"The 'illness/treatment' model has by its nature to emphasise what the patient cannot do rather than what he might be able to do; to emphasise that what requires to be done is carried out by others rather than what the patient might do for him/herself". p.262.
Power as exercised (degrees of freedom?) through the therapeutic turn: the history of therapies; social, industrial, occupational, physical, drama, psychotherapy et al. ...
Turner, V. (1969) The Ritual Process. Structure and Anti-Structure. Routledge, London. cited in Jennings, S. (1987) Dramatherapy and Groups, Chap. 1. pp.1-18. In Jennings, S. (Ed.), (1987) Dramatherapy. Theory and Practice for Teachers and Clinicians. Routledge, London. p.14.
Mitchell, R. (1987) Dramatherapy in In-patient Psychiatric Settings, Chap. 12. pp.257-276. In Jennings, S. (Ed.), (1987) Dramatherapy. Theory and Practice for Teachers and Clinicians. Routledge, London. p.14.
In theoretical terms, Mitchell also describes the creative model, the learning model and the therapeutic model (p.265).
Halifax, J. (1982) Shaman: the wounded healer. Thames and Hudson, London [England].
Born in Liverpool, UK. Community Mental Health Nurse NHS, Tutor, Researcher Nursing & Technology Enhanced Learning
Registered Nurse - Mental Health & General Community Psychiatric Nursing (Cert.) MMU PG Cert. Ed. BA(Joint Hons.) Computing and Philosophy - BIHE - Bolton PG(Dip.) Collaboration on Psychosocial Education [COPE] Univ. Man. MRES. e-Research and Technology Enhanced Learning, Lancaster Univ.
Live and work in NW England - seeking a global perspective.
The views expressed on W2tQ are entirely my own, unless stated otherwise. Comments are disabled. If you would like to get in touch please e-mail me at peter.jones AT h2cm.info
* IO Magazine
Source:
Reveal Digital , 01-01-1988
Contributed by: Charles Stein; Don Byrd; A.S. Yessenin-Volpin; Christer Hennix; Henry
Flynt; Henry Flynt; George Quasha; Charles Stein; Christer Hennix; Luitzen Egbertus Jan
Brouwer; L.E.J. Brouwer; L.E.J. Brouwer; Charles Stein
Stable URL: https://www.jstor.org/stable/community.28038534
Hodges' model was created by Brian E. Hodges [Senior Lecturer, Retired] in the mid-1980s at what is now Manchester Metropolitan University.
Peter Jones, author / editor of this blog has championed Hodges' model as a personal initiative online since 1998, but discovered the model on the CPN(Cert.) course 1988. The driver is recognition of the increasing relevance - decade-by-decade - of Hodges' model as a primary resource for local, national, global and glocal (virtual) health and education.
Visitors to this blog, individuals and organisations, are invited to consider use of Hodges' model.
Hodges' model is provided as an open educational resource (OER).
"Open Educational Resources are teaching and learning materials that you may freely use and reuse, without charge. OER often have a Creative Commons or GNU license that state specifically how the material may be used, reused, adapted, and shared." [Google, 8 Feb 2016]
CC CREATIVE COMMONS:
Hodges' model is assigned Attribution-ShareAlike 3.0 Unported (CC BY-SA 3.0):
OER is important for teaching, learning, and collaboration generally. Hodges' model is an ideal tool to span individual and global health care. Peter Jones encourages and will try to respond to support users interested in exploring how Hodges' model can support their work.
Post-publication I have learnt of new papers that have cited, or even used Hodges' model. This is very welcome news. If you are contemplating using h2cm, I'd be pleased to help. The aim is to see h2cm applied, especially in the real world, across disciplines and to help squeeze all the conceptual juice out of the model as per your context.
BIBLIOGRAPHY & Citations for Hodges' model
Please note the website - p-jones.demon.co.uk listed in many papers below is no longer available. 'Demon' ceased operating as an internet provider in 2015.
A new site for introductory materials and Brian Hodges' original notes will follow (one day!?) ...
Hodges, B.E. (1989) The Health Career Model, IN, Hinchcliffe, S.M. (et al.) 1989 Nursing Practice and Health Care, 1st Edition only, London, Edward Arnold.
Adams, T. (1987) Dementia is a family affair. Community Outlook, Feb, 7-8.
Jones, P. (1999) It's time to master the latest tools and Hodges' Health Career Model, IT in Nursing, 11.2.
Jones, P. (2004) Viewpoint: Can informatics and holistic multidisciplinary care be harmonised? British Journal of Healthcare Computing & Information Management, 21, 6, 17-18.
Jones, P. (2009) Socio-Technical Structures, the Scope of Informatics and Hodges’ model, IN, Staudinger, R., Ostermann, H., Bettina Staudinger, B. (Eds.), Handbook of Research in Nursing Informatics and Socio-Technical Structures, Idea Group Publishing, Inc. Chap. 11, pp. 160-174.
Kernohan, G. (2010) Theoretical review of public engagement in Nursing. Proc 1st Public Engagement Colloquium, Kells, Co Antrim, 22 April.
Murphy, K., Welford C. (2012) Agenda for the future: enhancing autonomy for older people in residential care.International Journal of Older People Nursing. 7, 75–80.
Jones P. (2014) Using a conceptual framework to explore the dimensions of recovery and their relationship to service user choice and self-determination. International Journal of Person Centered Medicine. Vol 3, No 4, (2013) pp.305-311.
Bom, J. (2015) Geboeid signaleren. De Verpleegkundig Specialist. 10. 14-15. 10.1007/s40884-015-0051-z.
Jones P. Exploring the relationship of threshold concepts and Hodges’ model of care from the individual to populations and global health. Rev Cuid. 2017; 8(3): 1697-720. http://dx.doi.org/10.15649/cuidarte.v8i3.464
Maffissoni, André & Vendruscolo, Carine & De Lima Trindade, Letícia & Zocche, Denise. (2018). Redes de atenção à saúde na formação em enfermagem: interpretações a partir da atenção primária à saúde. Revista Cuidarte. 9. 1-13.
Holmes, D. Perron, A. Jacob, J.D. Paradis-Gagné, É. & Gratton, S (2018). Pratique en milieu de psychiatrie légale: proposition d’un modèle interdisciplinaire, (Practice in forensic psychiatry: A proposed interdisciplinary model). Recherche en soins infirmiers, 134, 33-43. DOI: 10.3917/rsi.134.0033
Ashiquer Rahman, S.K. (2019) Mobilizing ePLANETe.Blue knowledge mediation portal to deal with new challenges of sustainable development in Higher Education and Research Etablishments (HERE) from a perspective of Knowledge Economy.
Thèse de doctorat de l'Université Paris-Saclay
préparée à l’Université de Versailles-Saint-Quentin-en-Yvelines. École doctorale n°578 Sciences de l’homme et de la societé Spécialité de doctorat : Sciences Économiques.
Hayward, B.A. (2020), Mental health nursing in bushfire‐affected communities: An autoethnographic insight. Int J Mental Health Nurs. doi:10.1111/inm.12765
Iris Lohja, Yves Demazeau, Christine Verdier. A multi-agent system approach to dynamic ridesharing for older people: State-of-the-art work and preliminary design. 18èmes Rencontres des Jeunes Chercheurs en Intelligence Artificielle, RJCIA’20, Jun 2020, Angers, France. pp.52-59. ⟨hal-02897446⟩
Byrt R. Forensic Mental Health Nursing in Secure Hospitals and the Criminal Justice System. Nurs Health Care Int J. 2019, 3(2): 000176.
Hamilton EAA, Dornan L, Sinclair M, McCoy J, Hanna-Trainor L, Kernohan WG. A scoping review protocol: Mapping the range of policy-related evidence influencing maternal health outcomes in a fragile, low-income country. J Adv Nurs. 2021 Jul 20. doi: 10.1111/jan.14956. Epub ahead of print. PMID: 34288043.
Elien G Neimeijer (2021) "CLOSE(D) CARE: Group climate in a secure forensic setting for individuals with mild intellectual disability." Radboud University, ISBN: 978-94-6416-713-9
https://www.trajectum.nl/sites/default/files/proefschrift_e._neimeijer_pdf.pdf
Fryer, Jon. “Information Literacies – Learning, to Thrive in a Digital Age” IRMS Bulletin 230 (2022): 16-21.
Kistler KB, Tyndall DE. Application of the Threshold Concept Framework in Nursing: An Integrative Review. Nurse Educ. 2022 Mar-Apr 01;47(2):91-95. doi: 10.1097/NNE.0000000000001041. PMID: 34033613.
Jones P, Wirnitzer K. Hodges’ model: the Sustainable Development Goals and public health – universal health coverage demands a universal framework. BMJ Nutrition, Prevention & Health 2022;0:e000254. doi:10.1136/bmjnph-2021-000254
Above paper cited by:
Leung, T.C.H., You, C.SX. (2023). Environmental, Social, and Governance (ESG) Promotion to Different Stakeholder Groups. In: Environmental, Social and Governance and Sustainable Development in Healthcare. Sustainable Development Goals Series. Springer, Singapore. https://doi.org/10.1007/978-981-99-1564-4_6
Yadav, V. S., & Singh, B. (2023). Evaluating the Human Rights Perspective on Sustainable Development Goals Accessible Health Coverage. Journal of Law and Sustainable Development, 11(6), e1254. https://doi.org/10.55908/sdgs.v11i6.1254
Kernohan, WG, Dornan, L & Jones, P 2023, 'A reflection on Hodges' Health Career Model for integration of health innovation', Trinity Health and Education International Research Conference 2023, Dublin, Ireland, 7/03/23 - 9/03/23.
McLaughlin, P., Brady, P., Carabellese, F., Carabellese, F., Parente, L., Uhrskov Sorensen, L., . . . Kennedy, H. (2023). Excellence in forensic psychiatry services: International survey of qualities and correlates. BJPsych Open, 9(6), E193. doi:10.1192/bjo.2023.578
[ For Dr Wirnitzer's work please see:
The NURMI-Study (NURMI – Nutrition and Running high Mileage) https://www.facebook.com/nurmistudy
Editorial: Situational Awareness, Psychoses, Cardiovascular Nursing, Research Methods and Hodges' model.
Hodges' model and the use of Diagrams in Case Formulation
Recognising the Value of Hodges’ model as a Known - Unknown in the time of COVID and Information Disorder.
Liberty Protection Safeguards, Threshold Concepts, Hodges' model in the Residential Care Sector (Parts 1 & 2)
Hughes (1958) is clearly dated, and as reflected in the title. Brian Hodges referenced Hughes to define ‘health career’ the idea of life chances.
Hughes, E. (1958) Men and their work. New York: Free Press.
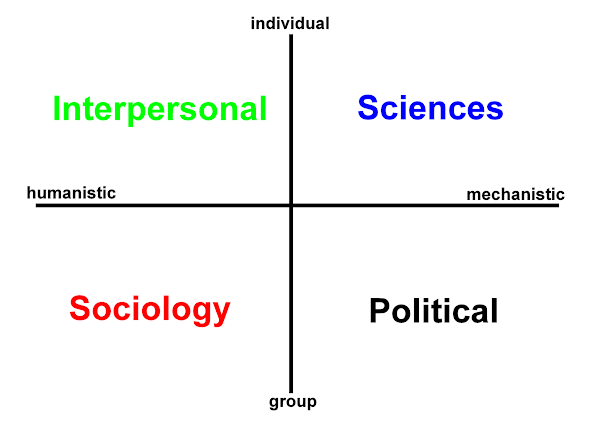
A paper in 1977 refers to "Health career model", this is not Hodges' model, but we can match the paper's econometric context as follows: 'health career' equates with 'life chances' and so draws upon the model's INDIVIDUAL domains. While in the paper "Life-cycle and Quality of Life" can be matched with the COLLECTIVE domains of Hodges' model, namely, SOCIOLOGICAL and POLITICAL. Of course, Quality of Life is also an individual, subjective, phenomenological experience. The paper however preempts the ongoing focus upon SOCIAL DETERMINANTS, and more generally, the current state of our Social and Political contracts. Now the further differentiation of political, commercial, geopolitical determinants (where we are born, what 'papers' we possess, or not; are we State/Stateless) is an opportunity for Hodges' model. The ability of Hodges' model to encompass and switch contexts provides evidence of the model's potential and power, a result of its structure and situated content. In health and social care, Quality of Life (clearly) remains an individual AND collective matter, from individual assessment tools, to weighing the ethics, benefits and costs of interventions in collective - aggregated terms (QALY).
"900: Welfare Programs; Consumer Economics; Urban and Regional Economics." (1977). Journal of Economic Literature, 15(4), 1451–1457. http://www.jstor.org/stable/2723014
The two papers below pre-date the first website [1998-2015 webarchived], but show how I have subsequently stressed the role of information, informatics and the socio-technical within Hodges model as a unifying concept. I have copious notes to revisit this subject, on: post-COVID and dis- mis- malinformation; and nursing's legacy issues.
Jones, P. (1996) Humans, Information, and Science, Journal of Advanced Nursing, 24(3),591-598.
Finally some software publications from the microcomputer era.
Jones, P. (1986) Computing in Nursing NEWS. Computerised Patient Assessment. Nursing Times. 85: 5. Sep 3-9;82(36):63-5. PMID: 3532039 (Describes 'CAPA', a BBC microcomputer program for student nurses.)
Jones, P. (1989) Computers in Nursing NEWS. Creating a Program. Nursing Times. Feb 1-7;85(5):66-8. PMID: 2648342 (Describes 'HAEM', a BBC microcomputer program for student nurses on blood and blood groups.)
Please contact me if you have a paper referencing Hodges' model, or you have a project in mind, but need some advice, more information to help you use the model. Thank you.
21th Annual STS Conference Graz 2023:
online
"Critical Issues in Science, Technology and Society Studies" 8th - 10th May 2023
https://stsconf.tugraz.at/
Information & Records Management Society: IRMS22 - Resilience, Recovery, Renewal
Glasgow - DoubleTree by Hilton, May 15-17 2022
8th Biennial Threshold Concepts Conferences
Online, 7–9 July 2021
Global Remote and Rural Healthcare
(Virtual) 17-18th November 2020
ATTENDED:
Systems: Transition to a Sustainable World 15th September 2023, Richmond Building, University of Portsmouth
RCGP’s 7th Health and Justice Summit: Journeys Through Justice – Leadership and Transformation
Bristol, 25-26 November 2019
Participant in Re-envisaging
Infection Practice Ecologies in Nursing through Arts and Humanities
Approaches RIPEN
Spring 2018 - October 2019
Threshold Concepts in Action, University of Dundee: 27th-28th June 2019
Friday 28th June 2019: Threshold Concepts in Health Special Interest Group meeting. Morning: papers/discussion with virtual access for members at a distance; Afternoon: research/writing workshop; sharing advice and ideas
Presented at UKSS Conference 2018
UK Systems Society: Can systemic thinking reshape health services?
Presented at 4th Int. Nursing Conference Jordan The Tipping Point: Creative Solutions to Health and Nursing Challenges
"نقطة التحول: حلول خلاقة للتحديات الصحية والتمريضية"
Is there interest in an open, accessible conceptual framework not only for self-care and health care but for planetary health too? I believe there is ...









 orcid.org/0000-0002-0192-8965
orcid.org/0000-0002-0192-8965